
A host of factors are putting a squeeze on primary care practices including rising paperwork demands, pay inequities, burnout, and insurer demands for prior approval. Federal regulators and legislators are pushing an increased role for telemedicine as one possible answer.
Get Instant Access to This Article
Subscribe to Worcester Business Journal and get immediate access to all of our subscriber-only content and much more.
- Critical Central Massachusetts business news updated daily.
- Immediate access to all subscriber-only content on our website.
- Bi-weekly print or digital editions of our award-winning publication.
- Special bonus issues like the WBJ Book of Lists.
- Exclusive ticket prize draws for our in-person events.
Click here to purchase a paywall bypass link for this article.
In late April, pharmacy giant Walgreens waved the white flag on its bold experiment in bringing frontline medical care into its retail spaces.
VillageMD primary care offices in Shrewsbury, Marlborough, and Framingham were among almost 200 across the country to shut their doors after Walgreens acknowledged its $5-billion bet in 2021 was yielding multi-billion-dollar operating losses in 2023.
“It’s not entirely surprising,” said Dr. Joahd Toure, senior vice president at UMass Memorial Health in Worcester.
Bringing care closer to the patient is a recurring theme in health care, Toure said, pointing to UMass Memorial Health’s own efforts to extend coverage into suburban villages and beyond.
Bringing a national brand name like Walgreens to the fight was a noble effort. But primary care is a tough nut to crack, Toure said. There aren’t enough doctors to go around, operating costs are rising, and margins are slim.
VillageMD still has about 500 clinics in operation in 26 markets apart from the Walgreens experiment.
Points of friction
A host of factors are putting a squeeze on primary care practices:
- Doctors complain rising paperwork demands are increasing costs and decreasing their ability to see patients;
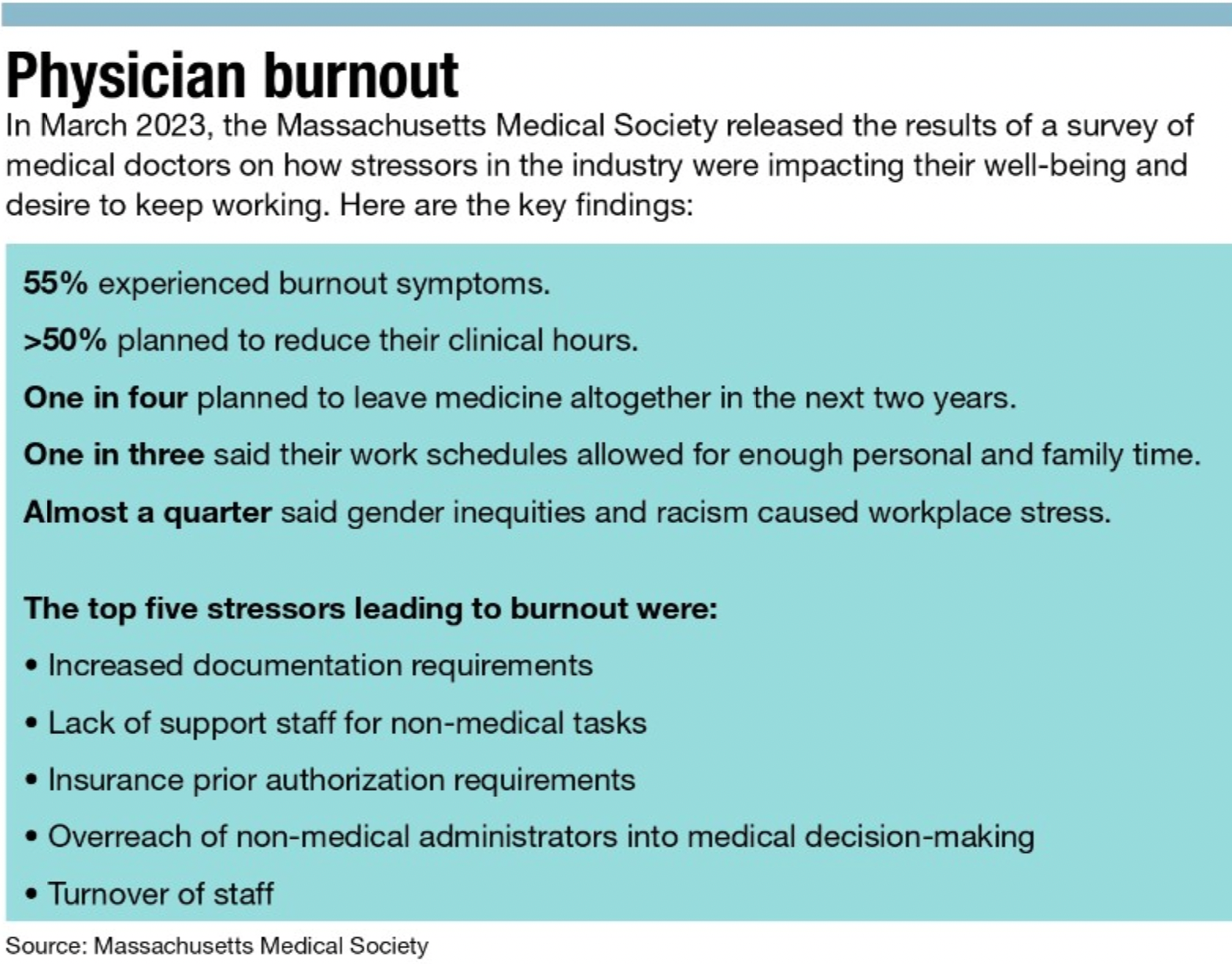
- Pay inequities and burnout are driving out primary care physicians;
- Insurer demands for prior approval on procedures, referrals, testing, and prescriptions is crippling;
- Baby Boomer doctors are retiring just as an increase in aging patients is hitting exam rooms.
Collectively, the situation demands new approaches.
Federal regulators and legislators are pushing an increased role for telemedicine as one possible answer.
Telemedicine came of age during COVID, Toure said.
“Now the toothpaste is out of the tube,” he said.
Medicare’s decision to cover telemedicine visits for primary and behavioral health is a game-changer. Efforts are underway in Congress to move telemedicine from a temporary measure to a permanent part of the solution.
Still, telemedicine has its limits, Toure said. Annual wellness visits need to be hands-on, for example. Routine endocrinology visits that involve evaluating tests results, by contrast, seem a good fit for telemedicine.
Certainly, a combination of in -person and online visits could be both effective and patient-friendly, he said.
Future of telemedicine
Telemedicine offers the prospect of doctors seeing patients outside the normal 8-to-5 office schedule, possibly by employing time-shifting techniques beyond state borders. He pointed to radiology, where imaging is read and evaluated in places like the Philippines and India, allowing work to continue while patients and doctors sleep in Central Massachusetts.
Could telemedicine eventually allow shifting weekend on-call coverage from overworked primary care doctors to perhaps a regional call center, restoring some work-life balance? Regulators in states like Arizona, Oregon, Florida, and Texas have cleared the way to erasing borders in licensing.
Asked if healthcare could follow banking into a technology trap, Toure demurred.
“I’m not a banker, and I don’t fully understand the business model,” he said. Looking at his smartphone, he acknowledged technology has made it easy to manage money without visiting a bank.
The banking industry went through a robust building period as it sought to bring services closer to customers only to find tech made branches redundant.
The blend of telemedicine and wearable technology constantly monitoring vital signs could reduce traffic to brick-and-mortar clinics. It could well play into expanded roles for physician assistants and nurse practitioners, another approach that can help in primary care. But those specialties are in short supply.
Bay State solution
In Boston, state legislators are looking at overhauling the funding of primary care through Senate Bill 750. That plan would double the funding ratio and eliminate co-pays for primary care.
The approach caught the attention of Dr. Frederic Baker, a solo practitioner in Holden employed by UMass Memorial Health.
As a past president of both the Massachusetts Academy of Family Physicians and the Worcester District Medical Society, he said both organizations have been actively lobbying on behalf of S.B. 750.

The bill calls for increasing state support for primary care from 7.6% of state healthcare spending to 12-15% and includes a fundamental shift to a direct, per-patient, monthly payment to providers. The concept could reduce healthcare inequalities.
The approach builds on the state’s historic leadership role in finding new approaches to healthcare issues, Baker said. And it keeps the state competitive with neighbors Connecticut and Rhode Island, which are hiking their funding commitments to primary care.
Most importantly, Baker said, it cuts to the heart of issues fueling a crisis in primary care.
He pointed to two telling datapoints:
1. More than twice as many anesthesiology residencies are available in the state (114) than family practice residencies (53). New doctors are steering away from primary care because of disparities in compensation, workload, and burnout, he said.
2. He’s seeing 12-14 patients a day in this practice, about a third of the number he was seeing in the early part of this century. His practice is maxed out, and he can’t accept new patients. The culprit, he said, is the complexity of paperwork requirements, from electronic records to insurer demands for prior authorizations.
Baker has been seeing patients in Holden for 30 years. That kind of continuity of care is an advantage clinics and urgent care facilities can’t match. He quickly ticks off cases where his history with the patient has led to a diagnosis others might have missed.
Still, he knows his solo practice model is the outlier in today’s world. While he thinks Senate Bill 750 can help level the playing field for primary care practices, the problems run deeper than compensation.
Price of paperwork
It takes 2.5 back-office staffers per physician to keep a practice running, he said. It’s costly, and finding good talent is difficult. The culprit is paperwork, even if technology has replaced paper and pen with check marks on a tablet.
“Reducing the administrative burden is a must,” he said.
One factor is state and federal regulatory requirements that micromanage in the name of safety and security. But a growing intrusion is insurers’ demands to pre-approve even the most routine testing and prescriptions.
Something has to change soon, Baker said. He urges patients to get involved in shaping the solutions by letting legislators know the importance of their relationships with their primary care physicians.